Delirium
A sudden, acute confusion
Definition
Delirium is an acute, varying severity of attention and consciousness disorder over the course of a day, as a result of a (serious) physical condition, drug poisoning (intoxication) or withdrawal from medication, nicotine, cannabis or alcohol. It is accompanied by:
- a disturbance in consciousness (reduced awareness of oneself or one's surroundings) that usually recovers
- a disturbance of attention and cognition (a reduced ability to direct, focus, maintain and shift attention)
- often with a perceptual disorder.
Characteristics of a delirium
- Acute confusion
- There is a change in (logical) thinking or in perception (altered cognition) the person does not think logically
- The severity of confusion can vary during the day one moment the confusion is worse than at another moment
(fluctuating symptoms) - The confusion occurs suddenly in a few hours or in a few days
- There is a change in (logical) thinking or in perception (altered cognition) the person does not think logically
- Memory problems the person forgets what was just said
- There is disorientation disorientation with regard to time, place or person
- Rapidly changing emotions the emotions and behaviour can also be completely different from normal for that person. For example, the person can be aggressive
- The person is bothered by external stimuli such as light and sound
- Incoherent speech the speech can be confused and unintelligible
- Attention problems the person cannot keep attention on what is happening or being said
- Questions have to be repeated. This is because attention is lost
- Previous questions have to be answered repeatedly
- Questions have to be repeated. This is because attention is lost
- Disturbed perception
- Sometimes there are delusions (imagining things that are not true)
- Sometimes there are hallucinations that can be frightening or strange (seeing, hearing or smelling something that is not there)
- You often see specific 'plucking' behaviour. The person plucks something that they see from the air or from the covers of the bed
- Sometimes there are delusions (imagining things that are not true)
- Reduced level of consciousness
- There is a reduced level of consciousness. It seems as if the person is not fully awake, nor asleep and at the same time is dreaming or having a nightmare.
- There is a reduced level of consciousness. It seems as if the person is not fully awake, nor asleep and at the same time is dreaming or having a nightmare.
- Restlessness or apathy Increase or decrease in psychomotor activity.
- The person moves more (motor restlessness) and is restless talking more than normal.
Ór - the person moves much less than normal and does less than usual or the person is sleepy, drowsy and apathetic. May lie in bed with the eyes open.
- The person moves more (motor restlessness) and is restless talking more than normal.
- Disturbed sleep-wake cycle There is difficulty staying awake during the day. During the day the confusion may be less and in the evening and at night even worse.
- Physical cause The confusion cannot be explained by an emotional mental disorder. Delirium is more common in patients in the hospital and is caused by one or more physical causes.
Three manifestations of delirium
- Anxious form (hyperactivity)
- Apathetic form (hypoactivity) This form is difficult to recognize. A person may seem quiet and absent. It is also called a silent delirium.
- Mixed form (both hyper- and hypoactivity)
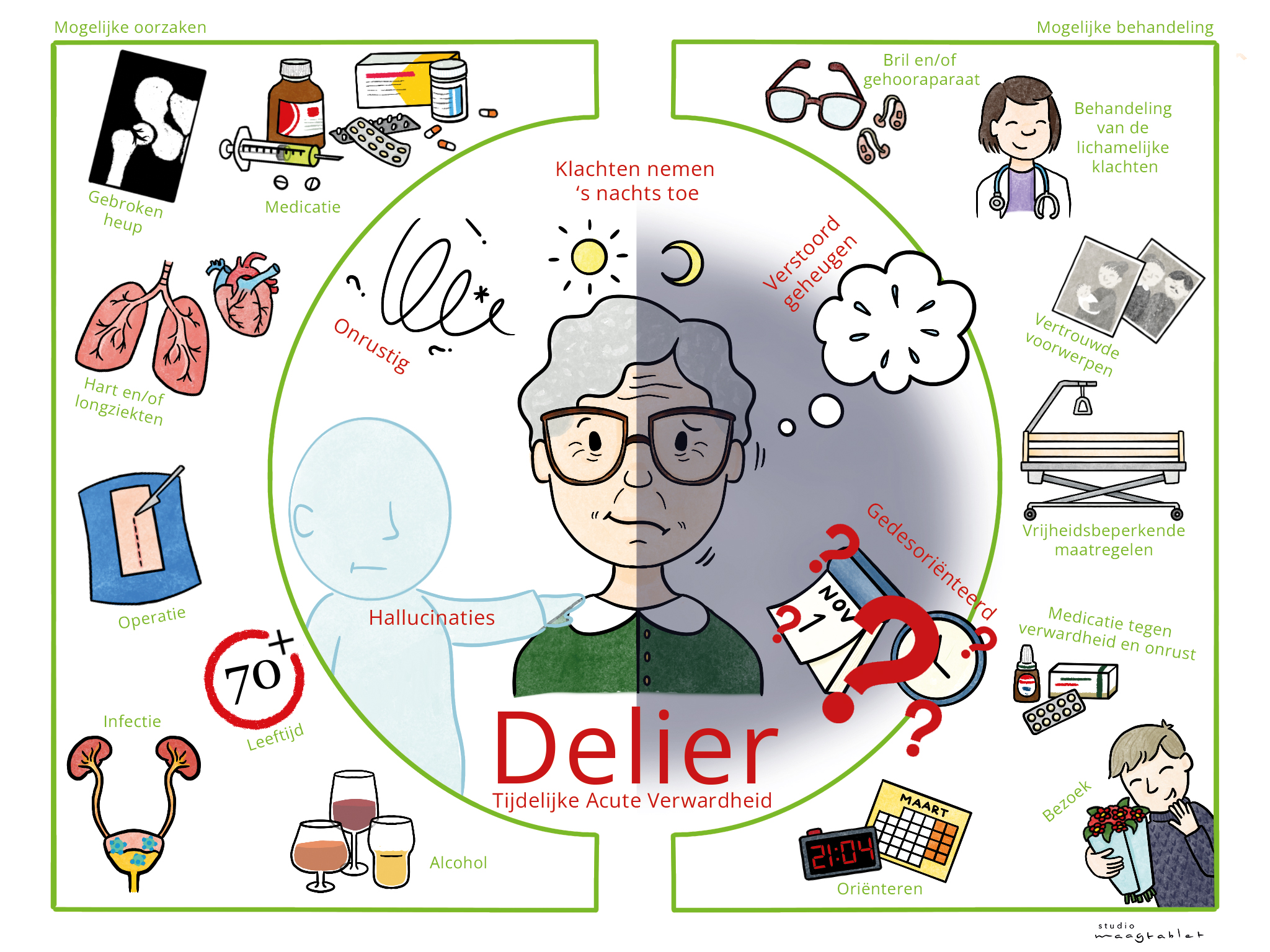
Causes of delirium / factors that can contribute to a higher vulnerability to delirium
In fact, a delirium is a disorder of the cerebrum and in particular a disorder of the brainstem. Anticholinergic medications, a disordered immune system and a disruption of the signal transmission in the brain seem to contribute to the development of delirium.
Brain injury related factors
- an acute traumatic brain injury. Almost half of patients with mild to moderate head injury (with a low GCS score) can develop a delirium in the first four days after the injury
- in the acute phase (first days) of a stroke / CVA, especially after an intracerebral hemorrhage, and specific injuries for example in the
thalamus and caudate nucleus - after brain surgery or surgery for a brain tumor
- after infections of the central nervous system such as encephalitis or meningitis and the mixed form meningoencephalitis
- after oxygen deficiency in the brain, for example after resuscitation, near drowning, respiratory arrest, prolonged epileptic seizure etc.
- after blood poisoning / sepsis
- after an acute encephalopathy
- after alcohol poisoning, alcohol abuse
- after COVID-19
There are probably more brain injury related factors, but they are not as well documented as the above.
General important factors
- age over 70 years, but delirium is not specifically age-related. Patients in an intensive care unit for children are also susceptible.
- existing reduced cognition / existing dementia. After a delirium has been experienced, a three-month wait is required before a suspicion of dementia can be diagnosed.
- alcohol abuse
- abruptly stopping drinking alcohol or abruptly stopping the use of certain medications (e.g. tranquilizers).
- psychiatric disorders
- the use of multiple medications (polypharmacy)
- poor vision (visual impairment)
- poor hearing
- too little sleep
- malnutrition
- physical disability
- an infection (for example a bladder infection or a sore throat or pneumonia)
- metabolic problems (for example due to a thyroid disorder, such as an overactive or underactive thyroid gland, an unregulated diabetes)
- chemical processes (for example due to anesthesia, or due to certain medications such as morphine, water tablets, medications with Prednisone, medications for Parkinson's disease, antidepressants, medications for heart rhythm disorders and medications for nausea or allergies, potassium deficiency)
- a fracture (for example a broken hip or arm), injury or accident, surgery
- heart or lung disease
- pain
- lack of sleep
- not being able to urinate properly from the bladder (urinary retention)
- malnutrition or dehydration (not drinking enough fluid or losing too much fluid)
- a blockage of the intestines
- an incurable disease in the final phase, (possibly due to morphine use)
- a previous history of delirium
Diagnosis
The gold standard for delirium diagnosis is currently still the fallible clinical judgment.
The first step is screening via validated screening lists for patients at risk, by trained professionals. The symptoms of delirium must be recognized after which the doctor makes the diagnosis.
Normally a DOSS is taken; DOSS stands for Delirium Observation Screening Scale. The patient's state of consciousness is measured three times a day with points. In addition to the DOSS, the AMT4, MOTYB and OSLA screening lists are also used. The OSLA also seems suitable for screening for delirium in patients with dementia.
See this Dutch page about delirium measurement instruments.
With a simple EEG measurement it is possible to diagnose delirium in Intensive Care patients. The pattern of brain waves in patients with delirium appears to be slower, more irregular and less complex.
A simple EEG with only three instead of twenty-one electrode patches can help make a diagnosis within one minute. However, medication can obscure the EEG.
This is all evident from the PhD research of technical physician Willemijn van der Kooi of the UMC Utrecht.
Research is still being conducted into whether examining blood and spinal fluid with biomarkers can be used.
Symptoms already present for a long time or suddenly occurring?
It is sometimes difficult to distinguish early dementia from delirium, because there is an overlap of symptoms. That is why diagnosing delirium is more difficult when dementia occurs simultaneously.
It is therefore also very important to know whether the symptoms have been present for a long time, or have suddenly occurred in a few days or hours.
Approach, do's and don'ts
The treatment of delirium consists of treating or removing the often physical cause of the delirium. The approach is equally important.
The patient with delirium has a great need for reality confirmation.
The environment should be as familiar as possible for orientation.
If the patient is hospitalized, make sure that there are familiar objects and familiar people.
Delirium can also be a stressful illness for a caregiver.
The caregiver needs a single point of contact from the professional team during the delirium. Explanation to the patient and to the caregivers in addition to the presence of an caregiver is therefore very important.
For orientation it is also important that when someone enters the room, he or she clearly and calmly states who he or she is. Speak in short sentences. Repeat if necessary. Limit the number of visitors, give rest and do not talk continuously. The familiar presence is more important than constant talking.
Show understanding and try to empathize and sympathize. If the patient screams in fear because something scary is seen in the hallucination, try to calm them down and tell them what you have observed. Ordinary objects can cause terrible fear, like in a horror film.
Someone can also see a butterfly fluttering or imagine another animal in the room.
Talk about familiar things, real events and real people. Reassure.
Provide a clear clock and show the date clearly. Provide good daylight during the day and a bedside lamp in the evening.
Provide a regular day and night rhythm.
Let as many permanent carers/nurses provide the care as possible, with as few changes of staff as possible.
Do not leave the patient unattended.
Treatment
It is important to determine an underlying physical cause and treat it. To increase reality, it is important that if the patient normally wears glasses or uses a hearing aid, these are given as soon as possible.
There is a greater chance of pressure sores (decubitus), ensure good alternating positioning. There is a greater risk of falling. If necessary, use a motion detector.
Exercise is advisable in itself, as is normalizing physical functions.
For treatment, we refer to the guideline database of Dutch medical specialists:
- Treatment with medication:
https://richtlijnendatabase.nl/richtlijn/delier_bij_ volwassenen_en_ouderen_2023/medicamenteuze_behandeling_van_het_delier.html
- Treatment without medication:
https://richtlijnendatabase.nl/richtlijn/delier_bij_ volwassenen_en_ouderen_2023/niet-medicamenteuze_behandeling_delier.html
For information in Engish, see the website of NICE (National Institute of Health and Care Excellence in the UK)
Recovery
A delirium usually recovers within a few days to weeks.
It varies from person to person. There are people for whom it passes, but that does not apply to everyone.
Elderly people in particular do not recover completely. It is possible that a patient functions less well cognitively after the delirium.
People can also be susceptible to experiencing a delirium again.
It is important to schedule an appointment at a delirium aftercare clinic three months after the delirium to discuss the experiences during the delirium and to determine the cognition.
It is generally assumed that the longer a delirium has lasted, the greater the consequences.
A delirium often leads to a longer hospital stay.
It causes a greater chance of developing dementia.
It appears that people who have experienced delirium are less able to cope at home after their admission. A delirium gives a greater risk of premature death
Resources
Hersenletsel-uitleg
samenvatting van de richtlijn: Delier bij volwassenen en ouderen (2020) https://richtlijnendatabase.nl/richtlijn/delier_bij_volwassenen_en_ouderen/startpagina_- _delier_bij_volwassenen_en_ouderen.html
https://www.medischcontact.nl/actueel/laatste-nieuws/artikel/simpele-eeg-meting-stelt-delier-vast
https://www.tergooi.nl/wp-content/uploads/2016/04/Folder-Delier-open-sans.jpg
{kind=link}
https://www.slideserve.com/clinton-walters/delier
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5317321/
Maneewong J, Maneeton B, Maneeton N, Vaniyapong T, Traisathit P, Sricharoen N, Srisurapanont M. Delirium after a traumatic brain injury: predictors and symptom patterns. Neuropsychiatr Dis Treat. 2017 Feb 14;13:459-465. doi: 10.2147/NDT.S128138. PMID: 28243098; PMCID: PMC5317321. https://pubmed.ncbi.nlm.nih.gov/37314306/
Garofano JS, Nakase-Richardson R, Barnett SD, Yablon SA, Evans C, Zaim N. Delirium following traumatic brain injury in adolescents: Symptomatology and prediction of ability to return to school or employment 1-year post-injury. PM R. 2024 Feb;16(2):122-131. doi: 10.1002/pmrj.13025. Epub 2023 Aug 17. PMID: 37314306.
https://pubmed.ncbi.nlm.nih.gov/34455093/
French J, Weber T, Ge B, Litofsky NS. Postoperative Delirium in Patients After Brain Tumor Surgery. World Neurosurg. 2021 Nov;155:e472-e479. doi: 10.1016/j.wneu.2021.08.089. Epub 2021 Aug 26. PMID: 34455093.
Kutlubaev MA, Akhmadeeva LR. [Delirium in the acute period of cerebral stroke]. Zh Nevrol Psikhiatr Im S S Korsakova. 2012;112(8):100-5. Russian. PMID: 23213851.
Al-Khaled M. Stroke-related delirium. J Neurol Sci. 2021 Jan 15;420:117250. doi: 10.1016/j.jns.2020.117250. Epub 2020 Nov 25. PMID: 33264682. https://pubmed.ncbi.nlm.nih.gov/17965033 / McManus J, Pathansali R, Stewart R, Macdonald A, Jackson S. Delirium post-stroke. Age Ageing. 2007 Nov;36(6):613-8. doi: 10.1093/ageing/afm140. Epub 2007 Oct 25. PMID: 17965033.
https://pubmed.ncbi.nlm.nih.gov/32055887/
Slooter AJC, Otte WM, Devlin JW, Arora RC, Bleck TP, Claassen J, Duprey MS, Ely EW, Kaplan PW, Latronico N, Morandi A, Neufeld KJ, Sharshar T, MacLullich AMJ, Stevens RD. Updated nomenclature of delirium and acute encephalopathy: statement of ten Societies. Intensive Care Med. 2020 May;46(5):1020-1022. doi: 10.1007/s00134-019-05907-4. Epub 2020 Feb 13. PMID: 32055887; PMCID: PMC7210231.
https://pubmed.ncbi.nlm.nih.gov/32193987/ Dittrich T, Marsch S, Rüegg S, De Marchis GM, Tschudin-Sutter S, Sutter R. Delirium in Meningitis and Encephalitis: Emergence and Prediction in a 6-Year Cohort. J Intensive Care Med. 2021 May;36(5):566-575. doi: 10.1177/0885066620913004. Epub 2020 Mar 20. PMID: 32193987.
https://pubmed.ncbi.nlm.nih.gov/33428871 / Pun BT, Badenes R, Heras La Calle G, Orun OM, Chen W, Raman R, Simpson BK, Wilson-Linville S, Hinojal Olmedillo B, Vallejo de la Cueva A, van der Jagt M, Navarro Casado R, Leal Sanz P, Orhun G, Ferrer Gómez C, Núñez Vázquez K, Piñeiro Otero P, Taccone FS, Gallego Curto E, Caricato A, Woien H, Lacave G, O'Neal HR Jr, Peterson SJ, Brummel NE, Girard TD, Ely EW, Pandharipande PP; COVID-19 Intensive Care International Study Group. Prevalence and risk factors for delirium in critically ill patients with COVID-19 (COVID-D): a multicentre cohort study. Lancet Respir Med. 2021 Mar;9(3):239-250. doi: 10.1016/S2213-2600(20)30552-X. Epub 2021 Jan 8. Erratum in: Lancet Respir Med. 2021 Jan 27;: PMID: 33428871; PMCID: PMC7832119.